The Hidden Cost Of “good Enough” Clinical Ai In Healthcare And Diagnostics
- 6 min read
Healthcare leaders rarely reject AI outright. What they reject is uncertainty. Over the past few years, many organizations adopted AI in a cautious, incremental way. Pilot projects. Narrow use cases. Limited exposure. That approach felt prudent. In 2026, it will start to look expensive.
The problem is not that healthcare organizations moved slowly. The problem is that many treated AI as a feature rather than a system. They added intelligence on top of existing workflows without rethinking accountability, validation, or operational control. That distinction is subtle early on. It becomes very visible at scale.
The result is a growing category of deployments that technically work but operationally fail. Models perform well in controlled tests but degrade quietly in production. Clinicians lose confidence. Compliance teams grow uneasy. Leadership concludes that AI is fragile, when in reality the operating model is.
Accuracy is not the same as safety
Most healthcare AI conversations still revolve around accuracy. It is easy to measure and easy to present. It is also incomplete.
In clinical environments, safety is not just about being right most of the time. It is about knowing when the system might be wrong, understanding why it produced an output, and having clear escalation paths when uncertainty crosses a threshold. A highly accurate model that fails silently is more dangerous than a less accurate system that fails visibly and predictably.
This is why explainability and governance are becoming structural requirements rather than regulatory checkboxes. Organizations are being asked to justify AI behavior not just statistically, but operationally. Who reviewed it. Under what conditions. With what controls in place.
Workflow gravity always wins
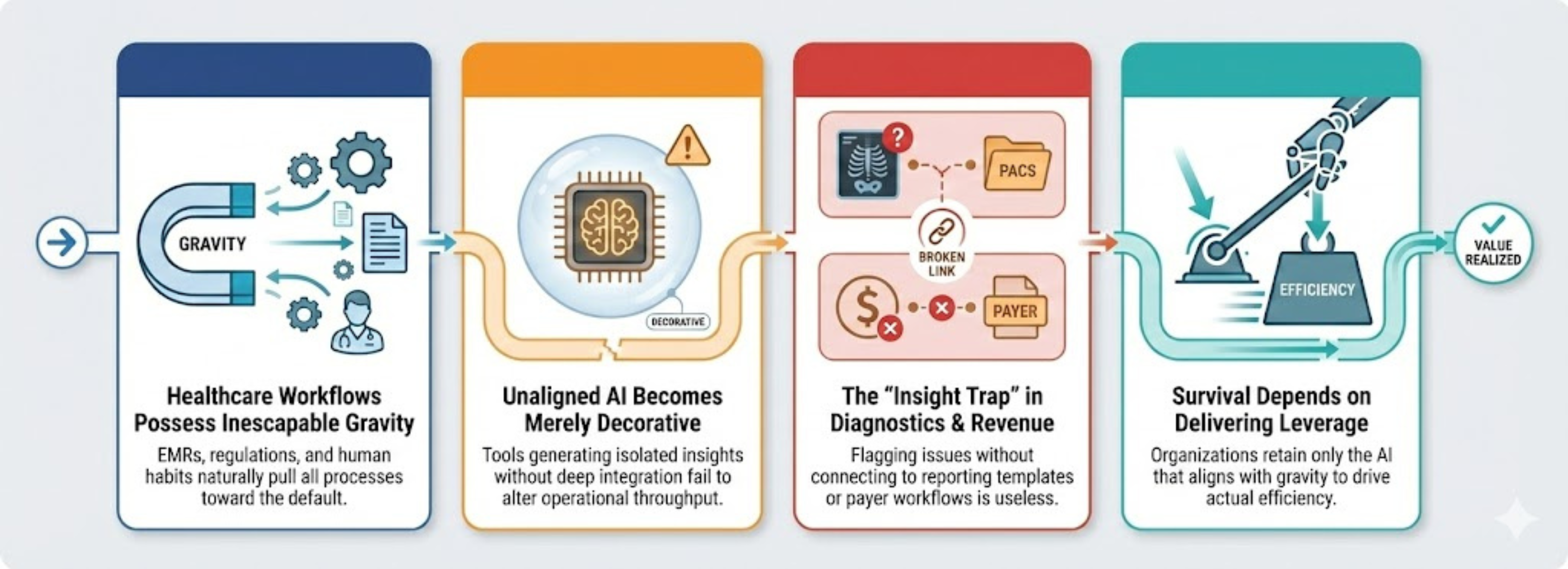
Healthcare workflows have gravity. Electronic medical records, clinical sign off processes, reimbursement logic, and human habits pull everything toward the default. AI that does not align with that gravity becomes decorative.
In diagnostics, this shows up when imaging AI identifies findings but does not integrate into PACS routing, radiologist prioritization, or reporting templates. In revenue cycle operations, it appears when prediction tools flag denials but do not connect to payer specific workflows or coder review steps. Insight is produced, but throughput does not change.
Organizations fund AI because they want leverage. They keep AI only when it delivers it.
The quiet risk of fragmented AI adoption
A two tier reality is forming in healthcare.
One group is treating AI as managed infrastructure. These organizations define ownership, validate continuously, monitor drift, and integrate AI deeply into workflows. AI becomes boring, which is exactly what production systems should be.
The other group accumulates disconnected AI tools. Each one looks reasonable in isolation. Collectively, they create blind spots. No single owner. No unified monitoring. No consistent governance. Risk is distributed until it is invisible.
In 2026, boards and regulators will ask harder questions. Where does AI influence clinical or operational decisions. How is performance monitored. What happens when behavior changes. If the answers are improvised, AI programs will stall or be rolled back.
From experimentation to operational trust
Three forces are accelerating this shift. AI is moving into higher impact workflows. Model availability is exploding, especially with generative and multimodal systems. Enterprise expectations around security, auditability, and measurable outcomes are hardening.
Together, they expose superficial adoption. Pilots that never matured into managed systems will not survive scrutiny.
The most effective organizations are reframing AI as a managed product capability. That means clear clinical ownership, technical ownership, defined change control, and explicit failure handling. Not as policy statements, but as working processes.
This is where delivery discipline matters more than vision. Engineering partners who emphasize production readiness, governance, and integration tend to outperform those who focus on novelty. Mobiloitte’s healthcare AI work reflects this quieter execution mindset, emphasizing compliance aware design, workflow integration, and long term operability rather than experimentation for its own sake.
The cost of waiting is not neutrality
Some leaders assume delaying AI adoption is the safest choice. In reality, the cost of inaction compounds. Operational inefficiencies remain. Workforce pressure increases. Data complexity grows. When adoption eventually becomes unavoidable, the gap is harder to close.
Healthcare organizations will not compete on who has the most AI features. They will compete on who can run AI reliably under real world constraints.
The question is no longer whether AI belongs in healthcare. It is whether your organization is prepared to operate it responsibly.
FAQs
1.What are healthcare AI solutions in practice?
They are AI systems embedded into clinical or operational workflows that change throughput, quality, or cost, not standalone analytics tools.
2.Why do many AI pilots fail after early success?
Because production conditions introduce data drift, workflow friction, and accountability gaps that were not addressed upfront.
3.Why is explainability important in healthcare AI?
Because clinicians and regulators must understand how and why outputs are generated in order to trust and govern them.
4.Is compliance enough to make AI safe?
No. Compliance addresses legal requirements. Safety requires monitoring, validation, escalation, and ownership.
5.Who should own clinical AI?
Clinical leaders must own outcomes. Technology teams must own reliability and integration. Shared ownership is essential.